Internal Assessment for 2011 International Review - CIHR Institute of Aging
Table of Contents
- Mandate and Context
- Institute Priorities
- Key Initiatives
- Transforming Aging Research
- Going Forward
- List of Acronyms and Abbreviations
- References
List of Figures
- Figure 1: Percentage of total CIHR expenditures in IA mandate areas, 2000–2010
- Figure 2: Specialization index and average of relative citations for top 10 countries publishing in cognitive impairment in aging, 2000–2008
Mandate and Context
The mandate of the Institute of Aging (IA) is based on the aging person in an aging society, and the effects of different diseases and conditions on aging. The Institute's goal is to improve the quality of life and health of older Canadians by understanding and addressing or preventing the consequences of a wide range of factors associated with aging. The Institute serves a diverse community of researchers in biomedical, clinical, health services and population health research. IA differs from many CIHR Institutes in that it focuses on aging from a developmental perspective rather than on particular diseases or functions. The Institute considers Canada's older citizens as important stakeholders in its knowledge creation and knowledge transfer.
Institute structure and operations
The IA office is situated at the University of British Columbia where a small administrative staff works closely with two Ottawa-based CIHR staff assigned to the Institute. An Institute Advisory Board (IAB) guides IA's work, with representation across research disciplines, government and policy makers, service providers, charitable organizations and older Canadians. The Institute's Scientific Director, Anne Martin-Matthews, will complete her appointment in July 2011, having led the Institute since 2004 through two successive terms. At that time the Institute leadership and operations will transition to a new scientific director and support team.
The Canadian context
As CIHR was being established, a need was recognized for strategic leadership and for the creation of a unifying centre for Canada's diverse research community in aging. Historically a small community, researchers in aging worked largely in isolation within single disciplines, disconnected from related work being done on their own campuses, much less across the country. In 1988, the National Task Force on Health Research presented to the interim governing council overseeing the design of CIHR, a case for the development of a Canadian Institute on Aging.Footnote 1
IA is unique within Canada as the sole national funder of strategic research that specifically targets aging.
National health charities are active and collaborative funders of research in aging as it relates to conditions such as stroke, arthritis and Alzheimer's disease. However, unlike the U.S. and UK, Canada has no charities that focus on aging per se.
IA operates at the government policy-research interface, working with senior officials from two federal government branches that have significant mandates for programs and policies affecting older Canadians: the Seniors and Pensions Policy Secretariat of Human Resources and Skills Development Canada, and the Division of Aging and Seniors of the Public Health Agency of Canada. IA also sits on the federal Interdepartmental Committee on Aging, engaging regularly with 24 government departments and agencies with responsibilities for seniors.
IA is the primary funder of health research on aging in Canada and stands as both a building and unifying force, driving research and knowledge exchange on priority issues in aging.
Institute Priorities
Strategic plans and priority areas
IA's first strategic plan was built on input from focus groups with key informants in four provinces, 42 personal interviews and internet-based consultations. These informed a Delphi process of priority setting by the inaugural Institute Advisory Board (IAB), led by Réjean Hébert, IA's first Scientific Director.
The plan, It's Time for Research on Aging (2002–2007), identified five priority areas sufficiently broad in scope to enable the Institute's overarching goal of building the research community in aging, while also advancing specific scientific themes:
- Healthy and successful aging
- Biological mechanisms of aging
- Cognitive impairment in aging
- Aging and maintenance of functional autonomy
- Health services relating to older people
IA supports research in all priority areas, but focused on two for its first strategic funding activities:
- Cognitive impairment in aging
- The Canadian Longitudinal Study on Aging (CLSA), covering all priority areas, but specifically addressing healthy and successful aging
In the period covered by this inaugural strategic plan, IA accomplished its developmental objectives by establishing itself as a national leader, strengthening the research community in aging and securing the foundations for the CLSA. IA's second strategic plan, The Future is Aging (2007–2012) was informed by:
- feedback received from the Institute's stakeholder community through CIHR's mid-term review, and expert recommendations from that review
- input from the Institute's regional research workshops held with seniors, policy makers and service organizations across Canada
- the IAB's review of IA's progress over its first five years, and assessment of how aging research in Canada had advanced, identification of emerging opportunities, appraisal of the nation's capacity to conduct research on aging and examination of the current environment and issues facing older Canadians
The priorities identified for 2007–2012 were to advance IA's leadership in cognitive impairment in aging and the CLSA, spearhead a strategic initiative on mobility in aging and augment three core drivers of research success: capacity building, knowledge translation (KT) and new alliances.
The 2006 International Review
The Institute was commended by the 2006 International Review Panel for its leadership in developing the Canadian Longitudinal Study on Aging, for multidisciplinary knowledge creation and for capacity building. The review panel reaffirmed the importance of further developing these and other endeavours, including KT and communications, partnerships and ethics. These were incorporated into IA's 2007–2012 strategic plan. The Institute's actions in relation to each are highlighted in later sections of this report.
Key Initiatives
Key Initiatives described in this section capture the Institute's strategic responses to unique needs in four areas of aging research: a national longitudinal data platform, enhanced research capacity, and science advancement in the two areas of cognitive impairment and mobility. The outputs and outcomes of these initiatives reflect their very different stages of development and maturation.
Initiative 1: The Canadian Longitudinal Study on Aging
Canada's need
The demographic realities of Canada's aging population are driving a need for cutting-edge programs of research that address health questions relevant to today's and tomorrow's older adults. Canadian researchers must be equipped to inform the policy and practice communities with evidence derived from complex inquiries into people's experiences, exposures, diseases and disabilities from mid-life to older age. This is optimally accomplished through a national initiative of significant sample size, multidisciplinary focus and longitudinal design.
Notice
The Canadian Longitudinal Study on Aging
The Canadian Longitudinal Study on Aging (CLSA) is a national study of adult development and aging individuals, each with unique experiences of their environments, communities, and health and social systems. Through the regular follow-up of 50,000 Canadians between the ages of 45 and 85 years over a 20-year period, the CLSA will serve as a research platform – a national data and biobank resource – that will accelerate understanding of the complex interplay among the vast array of determinants of health, from gene-environment interactions, to lifestyles, social networks and transitions in retirement and wealth. The CLSA's principal investigators, Parminder Raina (McMaster University), Christina Wolfson (McGill University), Susan Kirkland (Dalhousie University), more than 120 co-investigators and collaborators from 26 Canadian universities, are working together on this innovative multidisciplinary research program.
The Institute's strategy
IA has advanced the CLSA since the 2006 CIHR International Review on numerous fronts, most significantly:
- securing funding for protocol development, feasibility studies and implementation of the first five years of the CLSA
- overseeing the 12-member Ethical, Legal and Social Issues Committee guiding the CLSA
- building the case for the CLSA through the engagement of stakeholders across research disciplines, governments, agencies, health charities
- forging links with international experts to serve as advisors and collaborators
- guiding the establishment of terms and conditions for CIHR's oversight of this unique and major research initiative
The Institute of Aging has conceived the CLSA, nurtured its development and ensured its actualization. These have been achieved through actions that have garnered scientific buy-in from multiple sectors and secured substantial investments from CIHR and external partners to support CLSA's launch.
Outputs and outcomes
Remarkable achievements in the advancement of the CLSA have been made over the past five years by both the Institute and the principal investigators (PIs) of the CLSA itself.
The Institute's achievements
IA ensured rigorous scientific evaluation of the proposals and deliverables for each phase of CIHR funding for the CLSA. The Institute worked with CIHR staff to convene an international panel that reviewed the findings of CLSA developmental studies and assessed proposals for protocol development. IA subsequently made the case to CIHR's Governing Council and Scientific Council for funds supporting each of the developmental and implementation phases.
Through the CLSA Steering Committee, IA fostered a partnership with Statistics Canada to collaborate on its Canadian Community Health Survey, which in 2009 focused on healthy aging. This collaboration was critical to securing support from CIHR for the launch of the CLSA.
IA led a successful bid for CIHR operational resources to support a CLSA Ethical, Legal and Social Issues Advisory Committee, as well as the new position of CLSA executive director to manage the ever-increasing administrative complexity of the initiative. In 2008, IA led the formal negotiations with CIHR's Governing Council, scientific directors and executives to secure the crucial $23.5 million that financed the launch of CLSA's five-year implementation. IA's IAB recommended committing an additional $2.5 million (2010–2011 to 2012–2013) of its strategic funds to advance the CLSA – in particular, to accelerate data analysis and strengthen national research capacity in longitudinal health measurement and analysis.
The IA Scientific Director continues as the champion and strategic lead for the CLSA in all relevant discussions at CIHR. Her role is to ensure connections between the CLSA and other large research initiatives being developed, foster awareness of CLSA's value and utility as a national research platform and continually seek opportunities to enhance the operations of the CLSA.
Scientific achievements
The CLSA PIs and core research team have advanced longitudinal research knowledge by conducting eight feasibility studies assessing the logistics of the CLSA design and implementation across multiple jurisdictions and geographical locations. In addition to examining issues of sampling and cost, the CLSA team sought the perspectives of potential study participants on concerns such as frequency of contact, scope of data to be collected and data security. A special CLSA thematic issue of the Canadian Journal on Aging, September 2009, contains the resulting publications.
In June 2009, infrastructure funding was awarded to the CLSA following a highly competitive international review by the Canada Foundation for Innovation (CFI). The outcome was a $26 million grant: $10.2 million in federal funds and $15.8 million from provinces and other partners. With a Canadian investment of nearly $50 million, the CLSA has the resources to realize its proposed national network of core research facilities: a biorepository and bioanalysis centre, genetics and epigenetics centre, and statistical analysis centre, along with four computer-assisted telephone interview centres and 11 clinical data-collection sites across Canada.
The CLSA is "an outstanding national program of strategic importance...a significant research endeavour of a magnitude that...has not been seen before in population aging...a wonderful resource for decades to come in terms of factors which influence health in seniors...[and]...one of a kind even by international standards."
As of September 2010, the CLSA, in partnership with Statistics Canada, has obtained a sample of 12,000 individuals willing to participate in the longitudinal study. Even as participant recruitment and clinical protocol development has continued apace, the reputation and potential of the CLSA are being recognized:
- Federal government agencies, including the Public Health Agency of Canada and Veterans Affairs Canada are seeking to add measures to the CLSA protocol that will further enhance its utility to inform policy.
- The private sector is exploring public–private partnerships aimed at maximizing the transfer of CLSA findings into improved technologies and products.
- Not-for-profit organizations such as Neurological Health Charities Canada have expressed interest in partnering with the CLSA to help augment understanding of the chronic conditions associated with aging.
- CLSA's PIs are sought internationally for their insights on design and approach to longitudinal data collection and analysis.
The CLSA has become a multi-partnered major CIHR initiative with the full support of CIHR's Scientific Council and Governing Council.
The CLSA is poised to become the most significant accomplishment of the Institute of Aging.
Initiative 2: Building community capacity for research in aging
Canada's need
A skilled and vibrant research community capable of working across a range of disciplines to investigate complex issues is essential if scientific knowledge is to effectively address the needs of an aging population.
The Institute's strategy
IA defines capacity building as growing and strengthening the research community in aging by engaging scientists at all career stages and across disciplines in seeking answers to priority questions. IA recognizes that capacity building requires a variety of approaches responsive to unique goals and target groups. Capacity building has been an objective of the Institute since its inception and is identified as a key initiative in both of its strategic plans.
To ensure that the complexity of health and aging can be appropriately addressed through multidisciplinary perspectives, the IA's New Emerging Team (NET) grant program fostered research by new collaborators and their trainees from across disciplines and perspectives.
The NET program was recognized for its innovation and adopted widely by CIHR. Over its first five years, IA funded 14 NETs in all five of its priority areas of research. Outputs and outcomes of many of these are described throughout this report.
IA also established the CIHR Pilot grant program in 2002–2003, designed to serve multiple aging research capacity-development needs, including testing innovative and high-risk ideas, validating new tools and methods and testing new collaborations. These one-year grants also offer lower-cost opportunities for new investigators and those who have not previously focused their research on aging, to apply their expertise to questions relevant to this field. This is a core funding program for the Institute.
A third capacity-building goal of the Institute is to increase the number of trainees in aging research and expedite their development as scientists. In addition to funding a five-year Strategic Training Initiative in Health Research program on interdisciplinary research in aging (the Réseau de formation interdisciplinaire en recherche sur la santé et le vieillissement), a number of strategies have been successful in attracting, training and retaining new scholars in aging. These include:
- Trainee development as a critical element of all IA Team grants
- Top-up funding for the highest-ranked aging-focused recipients of CIHR salary and training support, and through select provincial partnerships
- Postdoctoral fellowships in IA strategic research areas such as longitudinal studies, cognitive impairment and mobility
- Prize programs that recognize and showcase excellence in publications, posters and podium presentations by trainees
- The annual IA Summer Program in Aging in which trainees practice skills essential for academic success while working and networking with future collaborators from across the country
External and internal partnerships are mechanisms by which IA leverages funds and strengthens research capacity. IA's partnerships serve to nurture the training of early career researchers in aging, enhance support to researchers in strategic areas and encourage scientists affiliated with other research domains to apply their expertise to issues of aging. This report highlights the scope and creativity of IA's partnerships with CIHR's institutes, branches and major initiatives, and with cross-council programs, allied agencies, professional organizations and international organizations. IA has been additionally enriched by its collaborations with two provincial agencies in aging research: the Réseau québecois de recherche sur le vieillissement, established in 1996 through the Fonds de la recherche en santé du Québec; and, in British Columbia, the Michael Smith Foundation for Health Research-funded BC Network for Aging Research (2006–2010).
By expanding, unifying and strengthening Canada's research community in aging, the Institute is ensuring availability of research relevant to our unique demographic, policy, cultural and geographic realities.
Outputs and outcomes
In discussing outputs and outcomes, this section will address growth in the research community in aging as well as the outcomes of capacity-building tools involving pilot grants, bridge funding and trainee support.
The number of researchers whose primary affiliation is with the Institute of Aging has, in 2010, shown a 12-fold increase over its first decade of operations; from 79 in 2000–2001 to 987 in 2009–2010.
While there are limitations to these data (possible multiple institute affiliation for any researcher, affiliation data based on non-validated researcher self-selection and a high proportion of researchers not identifying institute affiliation, particularly in the early years), they represent a significant increase in the number of scientists who self-declare an association with aging research or the IA.
IA purposely funds research in aging across all sectors of CIHR's scientific community. As an illustration, within 2009–2010 outlays, when expenditures with no single research theme identified are excluded ($1.5 million, representing 16% of IA expenditures), the distribution of Institute investments was 34.4% ($2.669 million) towards biomedical research, 33.4% ($2.624 million) to clinical research, 18.6% ($1.459 million) on health systems and services investigation, and 13.5% ($1.061 million) in social, cultural, environmental and population health research.
Figure 1 depicts the percentage of CIHR total expenditures being directed towards IA mandate areas. The increasing proportions across all grant and award categories since 2000–2001 are noteworthy. In 2000–2001, 6% ($15.6 million) and 4% ($1.4 million) of CIHR total expenditures were invested in open and strategic grants related to IA mandate areas, respectively. In 2009–2010, the proportion of CIHR grant expenditures in IA mandate areas rose to 13% for both open ($61 million) and strategic ($31.9 million) categories.
Figure 1: Percentage of total CIHR expenditures in IA mandate areas, 2000–2010
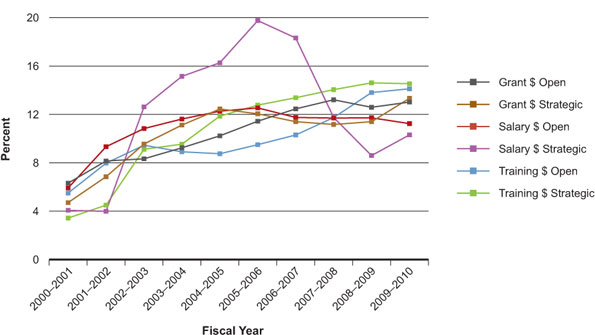
Salary award expenditures within IA mandate areas increased from 2000–2001 to 2009–2010, in both open ($1.5 million versus $2.1 million) and strategic ($150,000 versus $1.2 million) categories. As a proportion of CIHR total expenditures, IA mandate expenditures in open salary awards increased to 12% in 2003–2004 and have remained stable since. The proportion of strategic salary award expenditures, however, peaked at 20% in 2005–2006, and has since declined to 10% due to the elimination of a mid-career award in 2006–2007 in favour of other capacity-building strategies.
The data discussed are robust. However, some limitations should be noted. Funding data are based on a keyword search of the CIHR funding database and validated through a subjective process; and projects may have multiple institute affiliation.
Pilot grant funding
The Pilot grant program has been a key tool in building research capacity through mechanisms described previously. In addition to enthusiastic support for this program by funded researchers and application pressure that has increased almost five-fold (from 36 in 2002–2003 to 171 in 2010–2011) over the past eight years, evidence of the Pilot grant program success includes the following:
- Analysis of age data for 511 pilot grant applicants between 2002 and 2009 suggests investigators in their early years post-training are as successful in this competition as are researchers in later career stages.
- Analyses of the most recent three competitions (n=53 grants) shows that 58% of successful applicants were not primarily affiliated with IA. This suggests the program is meeting a capacity-building goal of fostering aging-related research by those from cognate areas.
- End-of-grant surveys of IA Pilot grant recipients from 2002–2003 through 2008–2009 (response rate: 93 out of 112 grantees), indicate the 40 PIs who have already applied for funding to support the next stage of their project have achieved a 50% success rate.
"This provided essential funding for us to determine the feasibility and sensitivity of our paradigms, both of which are necessary for submission for regular operating funds. We highly recommend the continuation of this program!"
Bridge funding
Bridge funding provides highly-ranked but unfunded applicants to CIHR's Open Operating Grant Program with one-year funding to enable research program continuity and grant application revision. Of the 46 recipients of these funds between 2003 and 2008, 26 (57%) went on to receive operating grant funding for the same project within one year. The typical success rate for the operating grant competition has averaged 26% over this same period.
Trainee support
Enhancing research capacity is an explicit requirement for IA's large team programs, which represent the Institute's primary route for trainee support. These team research environments are also highly effective in nurturing trainee success in CIHR open training and salary award competitions.
"Team grants allow us to plan ahead and recruit excellent trainees, work on a specific project, and help them with publications. This often leads to their success in open competition salary awards.... Our team grant funds for students always leverage additional funds."
In a complementary strategy, the Institute's support for individual trainees has been designed to bring an aging focus to allied fields of study, usually through a collaborative funding agreement. Examples of the Institute's external partnered trainee salary programs include:
- Veterans and Dementia Fellowship (with Veterans Affairs Canada)
- Focus on Stroke: Doctoral Research Awards and Fellowships (with the Heart and Stroke Foundation of Canada)
- Doctoral Research Awards in Occupational Therapy in Mobility in Aging (with the Canadian Occupational Therapy Foundation)
As a proportion of CIHR total expenditures, training award funding relevant to IA's mandate increased from 6% ($1.6 million) to 14% ($7.5 million) in the open category and from 3% ($105,816) to 15% ($2.6 million) in the strategic category between 2000–2001 and 2009–2010, respectively (Figure 1). Over the past five years the number of individuals conducting aging research who hold their own CIHR trainee award has almost doubled, from 203 in 2005–2006 to 375 in 2009–2010.
Recognition of excellence in aging research through prizes and travel awards is a mechanism by which the Institute encourages emerging scholars to take pride in their research in aging, while extending a sense of belonging to a vibrant and appreciative scientific community. Since 2001–2002, IA has awarded the following to master's, doctoral and postdoctoral trainees:
- 75 Age+ Prizes for excellence in research publication
- 29 Special Recognition Prizes for top-ranking applicants in open training and salary award competitions
- 20 Student Poster Prizes for best poster at the Annual Scientific and Educational Meeting of the Canadian Association on Gerontology
- 4 Réjean Hébert Prizes for best research presentation by a core program medical resident at the Canadian Geriatrics Society annual meeting
- 55 Travel Awards to present research on aging at scientific meetings
In a 2010 survey of trainees, of the 77 respondents who had received IA recognition over the past decade, 87% said that IA's support enhanced their motivation to continue research in aging and 82% indicated this support gave them confidence to apply for further awards and research funding.
"More than confidence... the prize can help others to determine my capacity."
Summer program in aging
IA's Summer Program in Aging (SPA) is a four-day annual retreat composed of plenary lectures and interactive workshops on peer review, writing successful grant proposals, interdisciplinarity, research communication and knowledge translation (KT), all within the theme of health and aging. Application pressure to SPA has doubled since its inception in 2006, with more than 120 applicants seeking 50 positions annually. IA has now co-hosted five SPAs with research centres in aging across the country, engaging a total of 250 master's, doctoral and postdoctoral trainees. Program evaluation has shown that SPA alumni consistently attribute elements of career success to their SPA experience.
"I learned skills at SPA that I apply every day in my position at McMaster, including writing and reviewing grants as well as the keys to publication success."
Ninety-two percent of the 119 SPA alumni responding to the 2010 IA Trainee Survey indicated the experience enhanced their motivation to continue research in aging, 85% said it made them feel more confident about applying for funding and 96% agreed it improved the skills they needed to be a successful scientist. Of the 49 trainees who participated in the first SPA in 2006, 11 have already received funding, either individually or as a research team co-investigator, amounting to more than $10 million from CIHR alone.
SPA has gained a reputation among Canadian researchers and their trainees as an outstanding mechanism for academic skill and personal development.
Initiative 3: Cognitive impairment in aging
Canada's need
As Canada ages over the next 30 years, the number of people with Alzheimer's disease or related dementias will increase from 500,000 to 1,125,000, with the subsequent economic burden rising from estimates of $15 billion to $152 billion per year.Footnote 2 The very close association of these conditions with aging led to an early agreement between IA and the CIHR Institute of Neurosciences, Mental Health and Addiction that cognitive impairment in aging, which includes Alzheimer's disease and related dementias, would be the one specific condition associated with aging to come under the aegis of IA.
The Institute's strategy
Recognizing Canada to be among the top 10 nations with respect to its contribution to global knowledge on cognitive impairment in aging (CIA), the Institute struck a two-pronged strategy to advance this research field.
The Institute founded the Cognitive Impairment in Aging Partnership in 2002 in order to address the priorities of a broader collective of stakeholders by leveraging small pools of CIA funding dollars held by a diverse group comprising health charities, professional associations and others. Collaborative research funding within the partnership targeted areas where Canada could accelerate its advantage or address unmet national knowledge needs. These were:
- Biological mechanisms and treatment of Alzheimer's disease
- Caregiving and care practice in cognitive impairment
- Vascular health and dementia
- KT in dementia
In addition to the CIA partnership, a range of funding mechanisms was opened to the research community through the Institute's positioning of CIA as one of its priority areas. Included were bridge funds, new emerging team grants and pilot grants.
Outputs and outcomes
Advancing knowledge
IA's direct influence on knowledge advancement in this field is largely through the Cognitive Impairment in Aging Partnership. Over the eight years of the partnership, IA has engaged 23 funders, most with little history of collaboration. IA's $5.59 million investment has resulted in a collective commitment of more than $32 million towards strategic research areas identified by the partners. These funds have supported the work of CIA scientists ranging from master's students to scholars ranked in the nation's top 10. These include Sandra Black (University of Toronto), who has advanced global understanding of vascular cognitive impairment, and Patrick and Edith McGeer (University of British Columbia), who broke new ground with their investigations on neuroinflammation and Alzheimer's disease.
Intensity and citation of scholarly publications across the scope of CIA are used here (in Figure 2) as standard measures of Canada's advancement of knowledge in this field.
The specialization index (SI) represents the relative intensity of publications by country in CIA research relative to the intensity of publications worldwide. As such, an SI value greater than 1.0 means that the particular country is more specialized in the priority area than the world average. The average of relative citations (ARC) represents the average number of citations received by papers over a two-year period following the publication year. An ARC value greater than 1.0 means the particular country's publications in the area are cited, on average, more frequently than the world average.
Figure 2: Specialization index and average of relative citations for top 10 countries publishing in cognitive impairment in aging, 2000–2008
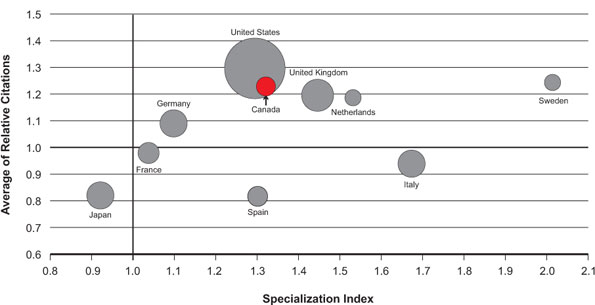
Figure 2 shows the ARC and the SI for publications in CIA among the top 10 countries for 2000–2008. Canada scores above the world average (1.0) on both indices (1.32 and 1.23 for SI and ARC, respectively). Furthermore, Canada ranks third among the top 10 countries for ARC, close behind the United States (1.29) and Sweden (1.24). Canada ranks fifth among the top 10 countries for SI. A steady increase in ARC from 1.18 in 2000 to 1.40 in 2008 indicates growth over time in citations of Canadian papers in CIA. The SI has fluctuated over time, but has consistently remained greater than the world average.
In Figure 2, the circle size relates to the number of publications produced in the research area between 2000 and 2008. Canada has a total of 2,256 publications, ranking seventh among the top 10 countries. Over time, there has been a steady increase in the number of Canadian publications in CIA, from 215 in 2000 to 298 in 2008.
Publications on CIA were identified through Medical Subject Headings searches done by the Observatoire des Sciences et des Technologies. Databases searched may not cover all publications in this area and ARC data are incomplete for 2008. Countries were ranked based on total number of publications over the time period.
Improving health and health services, informing decision making
IA's strategic funding programs in CIA have enabled its researchers to create knowledge that is improving the care of older Canadians. The following are a few examples.
Failure to recognize and appropriately treat delirium in older people arriving at the emergency ward puts patients' health in jeopardy. Jane McCusker (McGill University), funded through the Caregiving Grants in Cognitive Impairment in Aging, has tested and published Emergency Room directives for these high-risk presentations.Footnote 3
Rural seniors with dementia face an additional challenge of large distances between home and fragmented specialist services. With support of an IA New Emerging Team grant, Debra Morgan (University of Saskatchewan) and colleagues have tested the model of a Rural and Remote Memory Clinic as a "one-stop shop" where people with dementia can access all required specialist services in a one-day visit. Evidence for the feasibility and acceptability of this model led to ongoing provincial funding for this innovative clinic.Footnote 4
Policy recommendations on nutritional care of Alzheimer's patients are being published in the Journal of the American Medical Directors Association,Footnote 5 an outcome of work done through the IA-led Veterans and Dementia Fellowship program, in which Anne-Marie Boström brought her research expertise to a site of residential care for Canada's elderly veterans. Dr. Boström is continuing her international research collaboration with Canada, with her appointment in the Faculty of Nursing of the Karolinska Institute in Stockholm.
With an aging population, greater need is anticipated for chronic home care services across Canada. Janice Keefe (Mount Saint Vincent University), holds CIHR operating grant funding for the development of projections for Canadian human resource needs in chronic home care for elderly people over the next 30 years. Dr. Keefe is also a co-investigator with the Canadian Dementia Knowledge Translation Network.
Initiative 4: Mobility in aging
Canada's need
Mobility is a challenge for a significant proportion of the older population. In addition to external barriers such as poorly designed aids, transportation and built environments, older adults also cope with physiological and psychological barriers, such as musculoskeletal impairments and fear of falling. Fully 33% of Canadians over the age of 65 report having mobility problems, with the rate as high as 60% of those 85 years of age and over.Footnote 6 As baby boomers age, the economic and social costs of mobility impairments will be significant.
The Institute's strategy
In 2005, the Institute Advisory Board (IAB) approved Mobility in Aging (MIA) as a strategic focus for the Institute. This provided the scope to plan, communicate and fully execute a program of funding initiatives.
An eight-year, $20 million program of funding was developed to address the major research and KT gaps in mobility in aging. Consultations across traditional (e.g., musculoskeletal, neurological, clinical and social sciences) and non-traditional (e.g., engineering, housing and transportation) sectors of health research and their users helped define the following areas of focus for MIA:
- Understanding and defining mobility
- Maintaining and restoring mobility
- Measures, tools and technologies in mobility research and the assessment of mobility aids
- Supportive design covering housing, communities and transportation
Input from these consultations led to the requirement that all research projects funded within MIA have active user engagement from the outset. This was consistent with the KT objectives of IA's strategic plan, designed to ensure that the knowledge created is both useful and used.
Outputs and outcomes
Advancing knowledge
Early evaluation of the MIA initiative confirmed that the development funding was successful in expediting larger project grants. Of the 33 nominated PIs who received funding through MIA Development grants between 2005 and 2007, 39% proceeded to receive funding either as leads or collaborators on one or more of the nine MIA Emerging Teams and seven demonstration projects (a $15.6 million investment), and 35% were successful in other CIHR funding competitions for work relevant to mobility in aging.
"The MIA Planning and Development (P&D) grant enabled us to collect foundational data that informed the formation of a Wheeled Mobility for Older Adults Team grant. We are completing a video, which will act as a knowledge translation vehicle for the data. It has also led to our success in securing an emerging team grant in 2009."
Evaluation of themes funded under the MIA initiative at its midpoint identified significant national strength in research addressing three of the MIA research foci (understanding and defining mobility; maintaining and restoring mobility; measures, tools and technologies in mobility research and the assessment of mobility aids), specifically in relation to driving, falls, balance, gait, assistive devices and the emerging area of cognitive impairment–mobility interaction.
A dearth of inquiry into the supportive design research focus was also identified at the mid-point evaluation. IA has responded by launching a call for knowledge syntheses on topics associated with age-supportive built environments. In addition, the Institute provided select Canadian investigators and policy makers (from disciplines and sectors as diverse as medicine, urban planning, geography, kinesiology and health services delivery) access to advanced research and policy discussions in this area through a series of workshops in London (UK), Edinburgh and Montreal. Held in March and December of 2010, these meetings were brokered through partnerships between the Institute of Aging and the UK International Science and Innovation Unit, Canadian High Commission (London), Engineering and Physical Sciences Research Council (UK), Cities Institute (UK) and the Edinburgh College of Art. Significant success has already been achieved in the funding of a $1.5 million MIA Emerging Team grant, Walk the Talk: Transforming the Built Environment to Enhance Mobility in Seniors, led by Heather McKay (University of British Columbia) that includes several of these UK and Canadian collaborators.
At the policy interface, IA is aligned with the Canadian Association on Gerontology, the National Initiative on the Care of the Elderly and the Public Health Agency of Canada in the newly established Age-friendly Communities Canada Collaboration. The collaboration's objective is, through evaluation and research, to identify the evidence underpinning the World Health Organization's, and Canada's, Age-friendly Cities/Communities initiatives.
IA has also taken action to support further development of emerging themes in MIA. One example is the considerable research innovation evident among young Canadian scientists exploring the relationship between cognition and mobility. Teresa Liu-Ambrose (University of British Columbia) is assessing whether a recent history of falls is an early indication of cognitive dysfunction. Louis Bherer (Institut universitaire de gériatrie de Montréal) is examining the effectiveness of physical training and cognitive stimulation for improving mobility in frail elderly persons. In 2008, a full-day symposium on mobility and cognition convened by Manuel Montero-Odasso was hosted by IA and its partner, the Lawson Research Institute at the University of Western Ontario, assembling national and international expertise to exchange ideas and initiate collaboration.
Economic impacts, improving health, informing decision making
IA's Mobility in Aging strategy is just starting to generate knowledge that is being tested in the field. However, IA has a history of strategic support in mobility research, even prior to the launch of MIA, largely through its New Emerging Team (NET) program. Many of these NETs have already demonstrated impacts.
To alert those prone to falling when they're off balance, Brian Maki's NET (based at the University of Toronto) invented, tested and patented the Sole SensorTM, a simple shoe insert that uses a small raised ridge around its edges as a sensory warning. This product is now being distributed by Card Health Care, a privately owned Canadian company based in Ontario.
Bone degeneration and joint replacement are debilitating and costly realities associated with aging. The NET led by Rita Kandel (University of Toronto), co-funded by IA and the cross-cutting strategic initiative on Regenerative Medicine and Nanomedicine, focused on creating biomaterials for joint replacement. These materials allow treatment at earlier stages of degeneration, reduce or delay the need for joint replacement and ease the pressure on waiting lists.
Recognized as a global leader in the study of older drivers, the Canadian Driving Research Initiative for Vehicular Safety in the Elderly (CanDRIVE) team led by Malcolm Man-Son-Hing and Shawn Marshall (University of Ottawa) was initially funded by IA as a NET, and subsequently funded through CIHR's highly competitive Team grant program. This study has expanded internationally to Australia and New Zealand through an AUD$1.8 million, five-year Australian Research Council Linkage grant. CanDRIVE has contributed to provincial transport policies on driving and dementia prepared by the Canadian Council of Motor Transport Administrators and the Canadian Consensus Conference on Dementia. It has also informed the seventh edition of Determining Medical Fitness to Operate Motor Vehicles, a Canadian Medical Association publication used by physicians to help assess patients' fitness to drive.Footnote 7,Footnote 8
Transforming Aging Research
The Institute of Aging has made a significant impact on aging research and its translation in Canada. The following transformational initiatives have changed the national research landscape in aging.
The Canadian Longitudinal Study on Aging
The Canadian Longitudinal Study on Aging (CLSA) was developed to address important national and global knowledge gaps. Most studies of this kind focus on few and relatively specific constructs such as chronic disease or social determinants of health. Rarely do these studies consider molecular, genetic and cellular aspects of aging together with psychosocial aspects and variables such as nutrition, physical exercise and health services utilization. Extraordinary resources, cooperation across a host of sectors and political will are critical for the mobilization of research capacity, infrastructure and the operational funding essential for a project of this magnitude. The cost and organizational complexities of this essential tool for Canadian research innovation far exceeded the Institute's limited annual resources or any traditional CIHR funding model. The Institute of Aging led the way for subsequent cross-cutting initiatives by establishing a precedent and devising protocols for endeavours that transcend CIHR Institute purview. IA developed the case for CLSA through a series of strategic steps. The aim was to generate sufficient momentum through external interest and financial commitment so that the CLSA would ultimately be sustained and become operationally independent of IA.
International alliances in aging research
Recognizing the importance of collaborations with nations known for their excellence in aging research, and whose rate of population aging is similar to or more rapid than that of Canada, IA formulated an international partnership strategy in 2007. Collaborations with Japan and China, developed through CIHR-wide international agreements have given Canadian scientists a unique opportunity to collaborate in research that would not have been possible in Canada alone. This is illustrated by the work of Kenneth Rockwood and Arnold Mitnitski (Dalhousie University). With colleagues in China they are examining a clinical database of thousands of Chinese elderly, giving precision to algorithms that are being tested for accuracy of diagnostics for frailty and mortality.
IA negotiated its own partnership with the UK's innovative, multi-research council New Dynamics of Ageing programme. This Canada–UK Initiative is currently accelerating knowledge creation in productive and healthy environments for the older workforce, assistive technologies for nutrition and incontinence and connectivity of older adults in rural communities. Through this unique agreement with a novel partner, Canadian researchers are investigating multifaceted issues of aging with international experts in allied fields.
IA has initiated other collaborations with the UK, known globally for its expertise in mobility research, to include bilateral consultations on MIA priorities, co-funding (with the Engineering and Physical Sciences Research Council in the UK) a series of development workshops on age-supportive technologies in addition to the effective study tour described in the Key Initiatives section.
IA has also achieved status as an associate partner of the European Research Area in Ageing 2, participating in the FUTURAGE consultations to define the roadmap for aging research in Europe for the next 10–15 years, and advancing plans for collaborative trainee initiatives.
Lengthy negotiations with the U.S. National Institutes of Health–National Institute of Aging (NIA) led in 2006 to an innovative (USD$2.1 million) three-year partnership on postdoctoral funding through which, unfortunately, no applicants were fundable. Ongoing collaborations with NIA focus now on cognitive impairment in aging, through the International Collaborative Research Strategy on Alzheimer's Disease, discussed later in this report.
The Mobility in Aging Initiative
IA recognized that, unlike the well-developed community of CIA researchers, mobility in aging (MIA) researchers were disparate, often working in distinct silos. Some conducting MIA-relevant investigations did not identify their work with aging or health. To prepare this community for successful multidisciplinary team projects, a phased MIA funding trajectory was created: grants for research development and pilot work were offered initially, concurrent with announcements of annual rounds of larger MIA team and demonstration grants to be launched in succeeding years. This intentional sequencing and forecasting of funding opportunities enabled researchers to purposefully develop their investigative programs over the span of the MIA initiative. It also reduced the perception of risk for scientists in cognate fields who were entering aging research with complex multi-sectoral projects.
Knowledge translation
Through its 2007–2012 strategic plan, the Institute has set ambitious knowledge translation (KT) goals. These embrace a broad array of approaches to ensure that research on aging ultimately improves the quality of life and health of older Canadians.
Wide-ranging consultative processes with stakeholders now inform IA in its development of all strategic funding initiatives. Similarly, stakeholder involvement and other forms of KT are explicit requirements within all large strategic grants awarded by IA. One outstanding illustration is the IA-funded New Emerging Team under the leadership of Thomas Hadjistavropoulos (University of Regina), which not only resulted in the influential 2007 paper, An interdisciplinary expert consensus statement on assessment of pain in older persons,Footnote 9 but also led to a 2008 lay publication, Pain Management for Older Adults: a Self-Help Guide,Footnote 10 based on this team's innovative work.
IA offers grants for conducting KT, ranging in size and scope from the one-time $4 million Canadian Dementia Knowledge Translation Network (CDKTN) funding to research synthesis grants and smaller investments in programs engaging users in research development and dissemination. An example of the latter is IA's Outreach Initiative for NGOs (non-governmental organizations), which provides $10,000 grants for KT and research communications. Funded in the 2008 competition, Holly Tuokko (University of Victoria) and the British Columbia Psychogeriatric Association translated research evidence on older driver safety into a theatrical performance and instructional DVD and guidebook titled, No Particular Place to Go, currently being distributed across Canada.Footnote 11
The Canadian Dementia Knowledge Translation Network
Cognitive Impairment in Aging (CIA) partners recognized an urgent need to create capacity to better translate CIA knowledge and to enhance the stakeholder community's success in applying research knowledge. IA spearheaded the assembly of one national $4 million grant to address this need, engaging with CIA partners such as the Alzheimer's Society of Canada, the CIHR Ethics Office and Pfizer Canada. The successful application, the Canadian Dementia Knowledge Translation Network, is a collaboration of 22 universitiesand research hospitals, leaders in dementia-related research, Alzheimer's societies and care providers. The CDKTN has, among other accomplishments, launched a website repository for research information, educational and clinical tools, and event notices related to health services and caregiving for cognitively impaired elderly: http://www.lifeandminds.ca.
IA annually contracts one of its funded scientists or teams to host a symposium that involves researchers and research-users from across sectors, along with older members of the community, to discuss evidence and evidence needs in issues of health and aging. Topics have included frailty, the mobility–cognition connection and age-supportive built environments.
The scientific discoveries and the team research experiences of the 14 New Emerging teams (NETs) funded by IA, have been captured in a report aimed at improving team science in aging as well as transferring research knowledge. New Emerging Teams in Aging: Innovation and Impact (2009) continues to be distributed widely through direct mail, libraries and conferences.
Successful KT is now recognized annually through IA's $50,000 Betty Haven's Award in Knowledge Translation in Aging. This award, named in honour of a pioneer in aging research and KT in Canada, acknowledges outstanding KT activities designed to improve the health of aging or elderly individuals. The recipient of the 2009–2010 award is the Canadian Coalition for Seniors' Mental Health for their series of national guidelines and accompanying regional and provincial implementation strategies.
Through a small annual agreement ($10,000) with the Canadian Journal on Aging/La revue canadienne du vieillissement (CJA/RCV), the Institute has fostered the conversion of Canada's only bilingual aging-focused scholarly publication – which formerly had little reach outside the membership of the Canadian Association on Gerontology – to one that is widely indexed and distributed internationally and online through Cambridge University Press. The impact factor for the CJA/RCV has risen from .270 in 2004 to .738 in 2010 (source: ISI Web of Knowledge). Through this agreement, Institute-invited, peer-reviewed PROFILE articles are published in two issues of the journal annually. The CJA/RCV–Institute of Aging PROFILE is a platform for cross-disciplinary or cross-sectoral, widely accessible, commentary and analysis of current issues in aging and aging research. To date, articles have covered discussions on bridging research and policy, the importance of research on the biology of aging, the challenges of team science and ethics in aging research.
Citizen engagement
The 2006 International Review Panel recognized IA's innovative citizen engagement activities, specifically the five Institute-hosted Regional Seniors' Workshops on Research (RSWR), held between 2004 and 2006 as a knowledge exchange initiative with 300 seniors and those who work on their behalf. IA has analyzed, reported and taken action on what it heard during this extensive consultation:
- The priority research topic identified across all regions led to IA's 2009 adoption of its next strategic priority – health services and systems for an aging population.
- RSWR participants and other Institute stakeholders are now kept in contact with IA and abreast of Canadian research on aging through IA's electronic newsletter, Grey Matters, published and distributed three times yearly.
- IA invites select older members of the host community to serve on the judging panel for the Institute's student poster competition at the annual conferences of the Canadian Association on Gerontology. As stakeholder judges, they evaluate the KT merit of trainee work.
- The Institute appoints at least one older citizen as a lay representative on its IAB and, where feasible, facilitates citizen representation at Institute-partnered research consultations and KT proceedings.
- IA provides annual updates to the National Seniors' Council, which reports to three federal cabinet ministers.
- The Institute is adapting CIHR's Café Scientifique program in partnership with the Public Health Agency of Canada, inviting seniors' organizations to host café discussions with scientists and policy makers.
A highly successful project funded by a 2003–2004 IA Pilot grant tested methods of engaging seniors as researchers. One output is the 2010 publication, Grey Matters: A Guide for Collaborative Research with Seniors.Footnote 12 Written by Nancy Marlett and Claudia Emes of the University of Calgary, this book is a tool for seniors wanting to conduct their own research and for those aiming to involve seniors in research collaborations.
Going Forward
Emerging opportunities, expanding leadership
The next decade will provide an exceptional opportunity for CIHR and the Institute of Aging as attention is drawn increasingly to issues of population aging. For example, the 2010 Annual Report of the Chief Public Health Officer of Canada focuses on aging.Footnote 13 The federal government's Science, Technology and Innovation Council has identified "health in an aging population" as a research priority area where Canada can leverage research strengths to achieve a competitive advantage.Footnote 14
The research, policy and partnership implications of national demographics define a new era in Canada, giving unprecedented focus to issues of aging.
The Institute of Aging is poised to optimize opportunities in this new Canadian context and will lead CIHR in defining priorities. Many diseases falling within the mandates of other CIHR Institutes are progressively more prevalent with age. IA will guide the development of multi-institute research initiatives that address the complexity of coexisting chronic diseases experienced with aging. IA will also steer CIHR's engagement in emerging international collaborations to advance understanding of the relationships between growing older and getting ill.
In anticipating the challenges of providing health care to a population where one in four citizens is over 65, there is already escalating demand for research evidence of cost-effective policies, services and products. IA will further its alliances with provincial health delivery sectors, with CIHR Institutes whose mandates include population health and health services and with the CIHR Strategy on Patient-Oriented Research. The Institute of Aging has a leading role in defining the place of aging in relation to these emerging challenges and in driving national, CIHR and even Tri-Council priorities to address them.
As IA transitions its scientific director and Institute-based staff in mid-2011, the Institute's reputation as a leader is firmly grounded in its achievements, ensuring success going forward. This leadership will be sustained with guidance from a strong Institute Advisory Board (IAB), experienced Ottawa-based staff, committed stakeholders, and secure national and international partners.
Selection of new IAB members has been timed to ensure that members, including the board chair, will be relatively experienced and stable over the transition period. Strategic directions and funding commitments reach no more than a few years into the next administration's mandate, assuring continuity in Institute activity in the short term, but freedom for the next IA leadership to establish its own programs and processes.
Building on and supporting early initiatives
The Canadian Longitudinal Study on Aging (CLSA) – an IA achievement with the most striking potential for ongoing transformation of aging research in Canada – will need the Institute to champion its cause within CIHR. This will manifest as strategic support to the CLSA principal investigators and research theme leaders as they build alliances and forge national and international collaborations.
As the CLSA completes successive waves of data collection, IA's advocacy will become even more vital. The Institute must actively promote the alignment of CIHR funding opportunities and Roadmap priorities to fully optimize the exceptionally rich potential of CLSA as a legacy research platform. Developing and supporting harmonization and access to large population based data sets will also be central to the Institute's leadership role.
CIHR will undertake an evaluation of the CLSA in 2012 to determine funding and directions for years six to 10 of the proposed 20-year longitudinal study. IA will work to support the scientific leaders of the CLSA and help position it for the best possible outcomes of that evaluation.
The Cognitive Impairment in Aging (CIA) initiative has enhanced the breadth of research and opportunities for collaboration within this world-class Canadian research community. The results of a recent evaluation of CIA are being reviewed by the partnership and will shape future directions and funding collaborations. A challenge and an opportunity for IA will be to guide the CIA partnership in deciding how best to reposition itself in relation to CIHR's emergent International Collaborative Research Strategy on Alzheimer's Disease (ICRSAD). ICRSAD will establish Canada as a leader in Alzheimer's and related dementias (ARD) research by identifying common international priorities and support for scientific collaborations among researchers in Canada and internationally. Although CIHR has contracted scientific and operational leadership for ICRSAD, IA is the initiative lead within CIHR and will continue to champion the course of national and international ARD partnerships.
As the Mobility in Aging (MIA) funding outlay peaks in 2011–2012 and subsequently winds down, our experience confirms the need for ongoing Institute responsiveness to the field, its scientists and stakeholders. To enrich the work being done, IA must advance the connections among Canada's MIA research stars, explore emergent science and international opportunities, and foster the translation of new knowledge created by the MIA initiative. Already, MIA has built capacity in a previously diffuse research community in Canada and created a new generation of alliances, partnerships and research foci.
This report has emphasized commitment to development and support of research capacity as foundational to IA's activities and strategic initiatives. IA must sustain trainee development through a range of programs and help advance the careers of the more than 300 trainees it has already reached. Successful programs such as the Summer Program in Aging and recognition prizes are vital to the development of tomorrow's research scientists. As science becomes increasingly global, IA's programs must also strive to offer networking, training and collaborative research that reaches beyond national boundaries.
Addressing new priorities
Research on health services and systems has been one of IA's five priority areas since the Institute's inception. More than 200 projects related to health services have been funded by CIHR peer review committees in aging, and it has been a targeted funding area within the CIA partnership. IA has also been an enthusiastic partner with CIHR's Institute of Health Services and Policy Research and its creative, user-centered funding programs such as the Partnerships for Health Systems Improvement.
Following careful deliberation by its IAB in 2009, IA identified "health services and systems for an aging population" as its next strategic area of investment. This direction is informed by input from consultations with seniors groups across the country, by recognition of public and government attention to the emerging health care needs of the baby boom generation and their aging parents, and in alignment with CIHR Roadmap strategic priorities.
Currently, IA is undertaking partnership development activities and scoping work to identify priority research and knowledge translation opportunities, needs and gaps. We are collaborating with the Canadian Health Services Research Foundation on a series of regional workshops in fall 2010, partnering with the University of British Columbia's internationally recognized Centre for Health Services and Policy Research on a conference in February 2011, and identifying relevant information-gathering opportunities and processes. All of these will contribute to a discussion of priorities at IA's February 2011 and subsequent IAB meetings, as the Institute refines this broad and complex research area, identifies its niche and develops funding opportunities.
The way forward
CIHR Institutes are designed to enable the construction and operation of programs that will find answers to high-priority problems. Over the past decade, IA has learned much about the challenges and processes of initiating and leading a complex, cross-cutting strategic initiative such as the CLSA. These lessons will benefit the CLSA, other Institute programs and future CIHR major initiatives. Through its CIA and MIA programs, IA has also gained important insight into the diverse and thoughtful approaches required to engage partners and create strategic initiatives that reflect the nature and breadth of unique research and stakeholder communities. The MIA initiative has demonstrated the critical value of careful development and judicious launching of a package of theme-directed funding programs.
Building on experience, and taking into account recommendations anticipated from this 2011 CIHR International Review, IA will continue to strengthen the cadre of outstanding researchers and emerging scholars in aging funded in CIHR's strategic and open competitions. Research excellence and innovation will underpin all Institute activities as it leads and nurtures the research community in Canada and as it represents Canada to the world.
List of Acronyms and Abbreviations
CIHR Institutes
| IAPH | Institute of Aboriginal Peoples' Health |
| IA | Institute of Aging |
| ICR | Institute of Cancer Research |
| ICRH | Institute of Circulatory and Respiratory Health |
| IGH | Institute of Gender and Health |
| IG | Institute of Genetics |
| IHSPR | Institute of Health Services and Policy Research |
| IHDCYH | Institute of Human Development, Child and Youth Health |
| III | Institute of Infection and Immunity |
| IMHA | Institute of Musculoskeletal Health and Arthritis |
| INMHA | Institute of Neurosciences, Mental Health and Addiction |
| INMD | Institute of Nutrition, Metabolism and Diabetes |
| IPPH | Institute of Population and Public Health |
IA specific
| ARC | average of relative citations |
| ARD | Alzheimer's and related dementias |
| CanDRIVE | Canadian Driving Research Initiative for Vehicular Safety in the Elderly |
| CDKTN | Canadian Dementia Knowledge Translation Network |
| CFI | Canada Foundation for Innovation |
| CIA | cognitive impairment in aging |
| CJA/RCV | The Canadian Journal on Aging/ La revue canadienne du vieillissement |
| CLSA | Canadian Longitudinal Study on Aging |
| IAB | Institute Advisory Board |
| ICRSAD | International Collaborative Research Strategy on Alzheimer's Disease |
| KT | knowledge translation |
| MIA | Mobility in Aging |
| NET | New Emerging Team |
| NGO | non-governmental organization |
| NIA | U.S. National Institutes of Health – National Institute of Aging |
| P&D | Planning and Development |
| PI | principal investigator |
| RSWR | Regional Seniors' Workshops on Research |
| SI | specialization index |
| SPA | Summer Program in Aging |
- Date modified: